We help you regain your health and quality of life by treating various gynaecological conditions. Our experienced specialists provide a personalised approach, guided by the latest medical standards and gentle treatment methods.
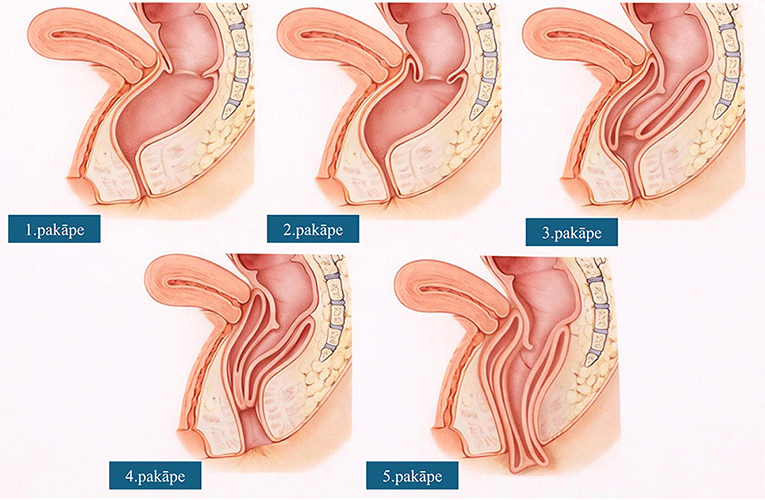
Rectal prolapse is a condition in which the rectum loses its anatomically normal position and descends downward, sometimes protruding even outside the anal opening. The anatomically correct position of the rectum is maintained by – the pelvic floor musculature and the anal sphincter complex, ligaments and connective tissues. In prolapse, these supporting mechanisms weaken. As a result, the rectum initially only slides into itself (so-called intussusception forms); as this progresses, the bowel may slip out through the anal opening. Five degrees of rectal prolapse are distinguished (Figure 1).
Figure 1. Degrees of rectal prolapse
Why does rectal prolapse develop?
The main risk factors for the development of rectal prolapse are:
chronic constipation and straining – frequent and prolonged straining during bowel movements increases pressure on the pelvic floor;
pelvic floor weakness – decreased tone of muscles and ligaments, which may be associated with age or trauma (e.g., birth trauma), and often combines with prolapse of other pelvic organs;
age – prolapse is more common in older people because tissue elasticity and muscle strength decrease over time;
female sex – each subsequent childbirth increases the risk of prolapse development;
childbirth – prolonged or difficult childbirth, a large fetus, use of vacuum extraction or obstetric forceps, and damage to pelvic nerves and muscles during the birth process contribute to the development of rectal prolapse;
chronic cough or physical overload – as a result, pressure in the abdominal cavity often increases, which also adversely affects the pelvic floor and pelvic organs;
previous pelvic operations or trauma – may affect supporting or nerve structures;
connective tissue weakness – may be congenital or acquired and is associated with reduced tissue resilience.
What are the symptoms of rectal prolapse?
Rectal prolapse is most often characterised by complaints related to bowel movements – chronic constipation or difficult defecation, a feeling of incomplete emptying after bowel movement and the need to visit the toilet repeatedly, and the need to use various assisting methods (enemas, manual mechanical assistance). As rectal prolapse progresses, faecal incontinence, mucous discharge or bleeding from the rectum, a visible or palpable protrusion from the anal opening, as well as discomfort or pain during bowel movements may develop. Rectal prolapse often combines with prolapse of other pelvic organs (uterine and vaginal prolapse, bladder prolapse or herniation of the small bowel into the pelvis), which may cause additional related symptoms (urinary incontinence, a feeling of heaviness in the perineum, vaginal dryness, etc.).
What examinations should be performed in cases of rectal prolapse?
In cases of rectal prolapse, the aim of examination is – to confirm the diagnosis, determine the type and degree of prolapse, assess functional disturbances, and exclude other pathologies.
For this reason, several examinations often need to be performed, and their combination may differ depending on the individual case; however, they can generally be divided into four main categories:
clinical evaluation – evaluation of complaints, determination of their severity (using assessment scales), physical examination (digital rectal examination at rest and during straining);
radiological examinations – defecography, colonic transit time, transrectal ultrasonography;
functional examinations – anorectal manometry.
What complications can rectal prolapse cause?
Rectal prolapse can cause both functional and anatomical complications, which over time may substantially worsen quality of life.
The most common complications are:
faecal incontinence;
constipation;
mucosal lesions and ulcers (cause bleeding or pain);
persistent mucous discharge and irritation of the perineal skin;
increased risk of urinary tract and gynaecological infections
In more severe cases, incarceration of the rectum may develop (when the prolapse protrudes outside the anal opening), followed by death (necrosis) of the intestinal mucosa or wall. Long-term untreated rectal prolapse may cause irreversible damage to the anal sphincter, persistent incontinence, significant deterioration in quality of life and social isolation.
What is the treatment of rectal prolapse?
Treatment of rectal prolapse depends on the type and degree of prolapse, symptoms, the patient's age and general condition. Treatment is mainly surgical. In early stages of prolapse (1st and 2nd degree) or in patients with high operative risk, conservative treatment is used (diet and lifestyle correction, use of laxatives, pelvic floor rehabilitation), which may reduce symptom severity but not cure the prolapse. Two approaches are used in surgical treatment – abdominal surgery or surgery with a perineal approach.
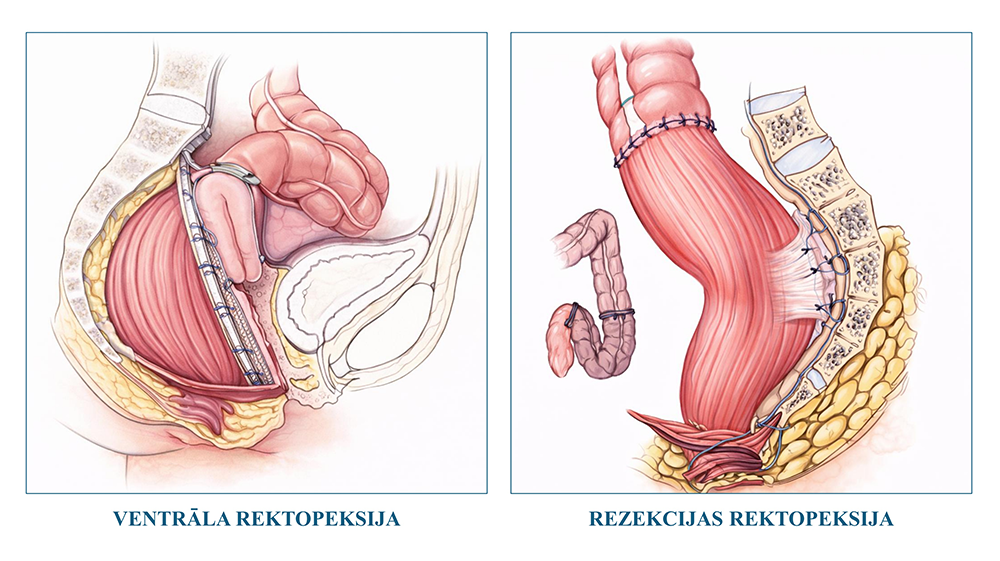
Abdominal surgery is performed laparoscopically, and it has two modifications (Figure 2):
ventral rectopexy – the rectum is fixed to the sacrum with the help of a synthetic mesh (used most often);
resection rectopexy (Frykman-Goldberg procedure) – excision of the sigmoid colon and fixation of the rectum are performed (in selected cases).
Figure 2. Rectal prolapse correction operations using an abdominal approach.
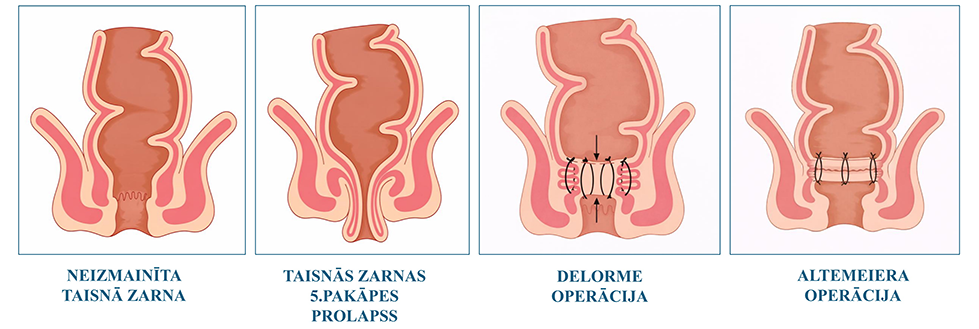
In an operation via a perineal approach, two modifications are used (Figure 3):
Delorme procedure – removal of the prolapsed mucosa and plication of the rectal muscular layer;
Altemeier procedure – full-thickness excision of the prolapsed part of the bowel and creation of a new bowel connection (anastomosis) in the anal canal.
Figure 3. Rectal prolapse correction operations using a perineal approach.
This website uses strictly necessary cookies to function. With your consent, statistical and social media cookies may also be used on this site.
Funkcionāls
Always active
Tehniskā glabāšana vai piekļuve ir noteikti nepieciešama leģitīmam mērķim, lai ļautu izmantot konkrētu pakalpojumu, ko skaidri pieprasījis abonents vai lietotājs, vai tikai ar mērķi veikt sakaru pārraidi elektronisko sakaru tīklā.
Settings
Tehniskā glabāšana vai piekļuve ir nepieciešama leģitīmam mērķim saglabāt preferences, kuras nav pieprasījis abonents vai lietotājs.
Statistika
The technical storage or access that is used exclusively for statistical purposes.Tehniskā krātuve vai piekļuve, kas tiek izmantota tikai anonīmiem statistikas nolūkiem. Bez tiesas pavēstes, jūsu interneta pakalpojumu sniedzēja brīvprātīgas atbilstības vai papildu ierakstiem no trešās puses, informāciju, kas tiek glabāta vai izgūta tikai šim nolūkam, parasti nevar izmantot, lai jūs identificētu.
Mārketings
Tehniskā uzglabāšana vai piekļuve ir nepieciešama, lai izveidotu lietotāju profilus reklāmas nosūtīšanai vai lai izsekotu lietotāja darbībām tīmekļa vietnē vai vairākās tīmekļa vietnēs līdzīgiem mārketinga mērķiem.