
Gallstone disease, or cholelithiasis, is a disorder of the digestive system associated with metabolic disturbances, characterised by the formation of stones (concrements) in the gallbladder or bile ducts due to changes in the composition of bile (with cholesterol and calcium bilirubinate playing the main role). Initially, small crystals form within the bile and settle on the wall of the gallbladder. Over time, they increase in size, forming stones (Fig. 1). The size of gallstones most commonly ranges from 0.5 to 2 cm, although they may be larger. The largest gallstone described in the literature measured 16.8 cm, which is rare. The composition of gallstones may vary depending on their cause: cholesterol stones (80% of cases); calcium, bilirubin and pigment stones (10–20% of cases); and mixed stones (comprising a combination of the two types mentioned above).

Gallstones
There are several risk factors that contribute to the development of gallstone disease: female gender, age over 40, ethnicity (European or Native American origin), pregnancy, obesity, type 2 diabetes mellitus, insulin resistance, hypercholesterolaemia (elevated blood cholesterol levels), prolonged fasting, rapid weight loss (due to dieting or bariatric surgery), a diet high in fat and low in fibre, heredity (~25% of cases), Crohn’s disease, and patients following extensive burns, trauma or spinal cord injury with subsequent paralysis.
The gold standard for diagnosing gallstone disease is abdominal ultrasonography (ultrasound), which is a minimally invasive, safe and sensitive method. It allows detection of bile thickening, which is often a precursor to gallstone disease, as well as gallstones larger than 2 mm. Gallstone disease is also frequently detected by abdominal computed tomography; however, compared to ultrasound, this method cannot fully exclude the presence of gallstones, as cholesterol stones (which are the most common type) are not visualised using this radiological method.
Gallstone disease may be an incidental finding and cause no symptoms; however, its presence increases the risk of complications associated with gallstones. The most common manifestation is a feeling of heaviness or pain in the right upper abdomen or upper abdominal region after eating. The pain may be dull and prolonged or colicky (biliary colic), radiating to the right shoulder or back. Nausea and vomiting may also occur.
The types of complications are often determined by the size of the stones. Small stones most commonly cause complications related to their migration and obstruction within the bile ducts at various levels, whereas larger stones more often lead to acute or chronic inflammation of the gallbladder wall or, less commonly, pressure necrosis.
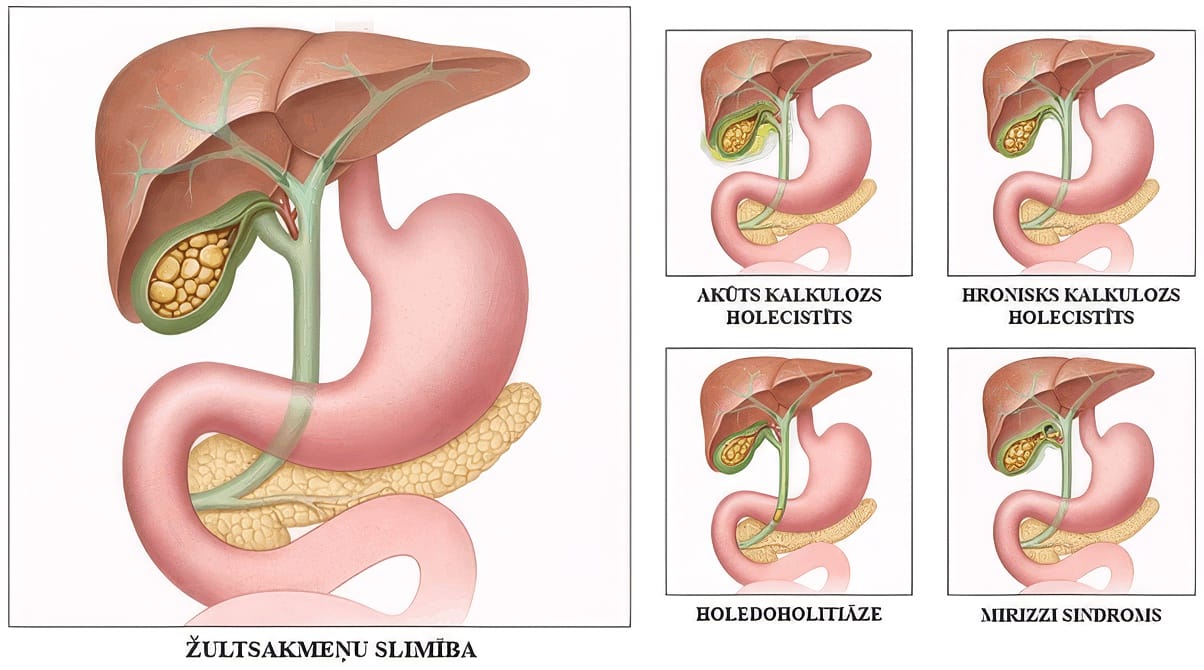
Complications of gallstone disease.
In cases of symptomatic gallstone disease, surgical treatment is indicated – laparoscopic cholecystectomy (removal of the gallbladder together with the stones). The operation is performed under general anaesthesia using a minimally invasive approach. During the procedure, an optical instrument is inserted into the abdominal cavity to visualise the organs, and the surgery is carried out through additional small incisions (Fig. 3). If stones have already formed in the gallbladder, it cannot be preserved. The main function of the gallbladder is to concentrate and store bile, which is released during meals; however, it is not considered a vital organ, as the bile ducts continue to function after its removal. In 10–25% of cases, so-called post-cholecystectomy syndrome may develop, characterised by gastrointestinal symptoms of varying severity (nausea, a burning sensation or intermittent abdominal pain, flatulence, diarrhoea, intolerance to fatty foods). However, pronounced symptoms affecting quality of life occur in only around 2% of cases.
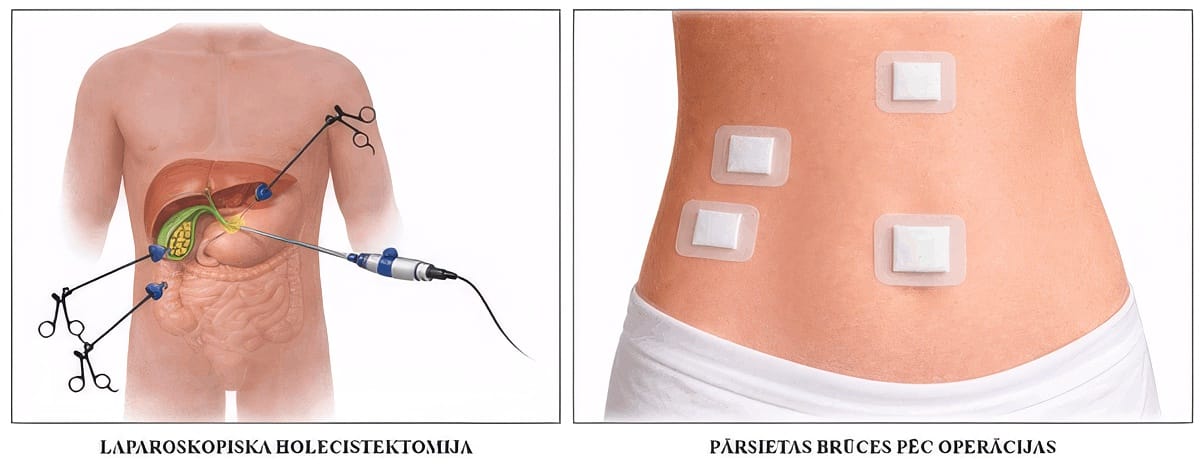
Surgical treatment of gallstone disease.
One of the treatment options for gallstone disease is pharmacological therapy with ursodeoxycholic acid. However, this approach is only suitable in cases where the stones are very small and composed solely of cholesterol. The duration of treatment is approximately 6–18 months, and throughout this period there remains a risk of symptoms and complications associated with gallstones. In addition, it has been established that the risk of recurrence within 5 years after treatment is around 50%. Due to these limitations and its relatively low effectiveness, this approach is not widely used.
In cases of asymptomatic gallstone disease (when gallstones are detected on ultrasound but the patient has never experienced related symptoms), a watchful waiting approach is acceptable until the first symptoms appear. However, it should be noted that approximately 25% of patients with gallstones develop symptoms or the aforementioned complications within an average of 10 years. In certain cases (calcification of the gallbladder wall, stones larger than 2–3 cm, and other rare medical conditions), surgical treatment is recommended even in asymptomatic cases.
In all cases of gallstone disease, a consultation with a surgeon is recommended in order to determine the most appropriate treatment strategy.









CALL US:
+371 26 412 412WHATSAPP:
+371 26 412 412
If you have been diagnosed at another clinic, call us to book a preoperative consultation –
we will offer you the earliest available appointment.
SEND US A MESSAGE

