
Colonic diverticulosis is a condition in which small sac-like protrusions (approx. 3-10mm in size) form in the wall of the colon in areas where the muscular layer of the intestinal wall is weakened (Figure 1). Weakening of the muscular layer is associated with ageing (as a result, tissue strength and elasticity change), chronic constipation and a low-fibre diet (as a result, the frequency of passage of intestinal contents decreases and pressure in the intestine increases). Diverticula most commonly develop in the descending colon and sigmoid colon, which is related to physiological characteristics – toward the terminal part of the digestive tract, pressure inside the intestine increases, facilitated by intestinal peristalsis (movements). Nevertheless, diverticulosis may also develop in any other part of the colon. The association between the development of diverticulosis and diet is also supported by its prevalence in different populations – e.g., in North American countries, in people after 60 years of age it is found in up to 50%, whereas in Asian countries it is found in only around 1%.
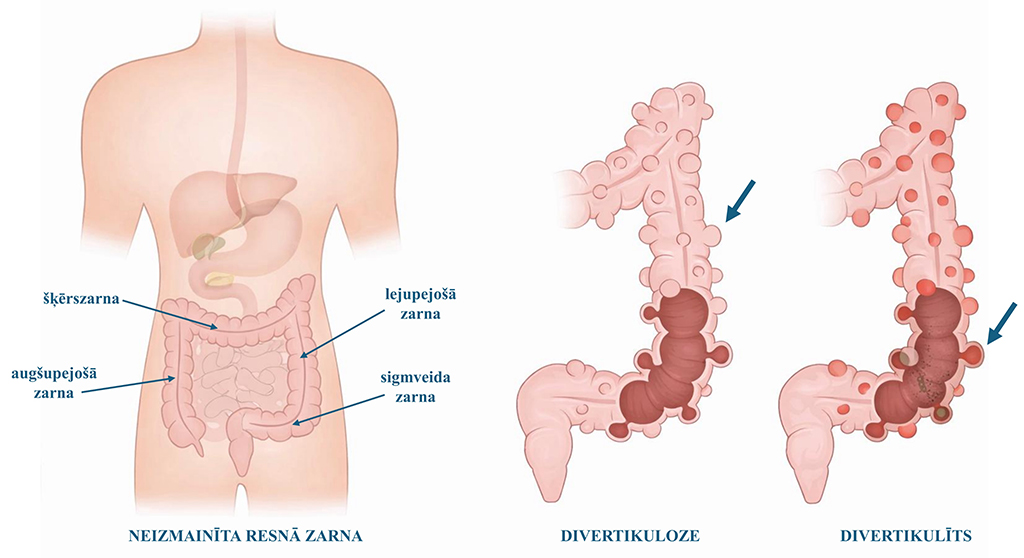
Diverticulitis is acute inflammation of the colonic wall that develops in the area of a diverticulum (Figure 1). This inflammation is most commonly caused by undigested food particles or faecal fragments (in the case of hard stools), which obstruct this sac-like protrusion in the intestinal wall; as a result, inflammation develops and the normal intestinal microflora proliferates, promoting the development of infection in this area. Although diverticulitis most often affects elderly people (more often women), it is nevertheless found in ~20% of cases before 50 years of age (more often in men).
Diverticulosis does not cause symptoms unless inflammation (diverticulitis) has developed. Nevertheless, the term “diverticular disease” is described, which is characterised by various gastrointestinal symptoms, e.g., periodic abdominal pain, meteorism (abdominal bloating), changes in bowel movements (constipation or diarrhoea). These symptoms are non-specific and overlap with symptoms of irritable bowel syndrome, and it is often difficult to differentiate them.
In diverticulitis various acute symptoms are characteristic, the severity of which depends on the severity of inflammation. Depending on the course of diverticulitis, it is classified as uncomplicated or complicated diverticulitis.
| Acute uncomplicated diverticulitis | Acute complicated diverticulitis |
| • Usually manifests with localised pain in the lower left abdomen, which starts gradually and worsens over several hours or days. • Changes in bowel function are often observed – constipation or diarrhoea, abdominal bloating. There may be loss of appetite, fever, and nausea. • Symptoms are usually mild to moderate. | • A situation in which inflammation-related complications have developed – acute bleeding, intestinal obstruction, perforation (rupture) of the intestinal wall with development of local or diffuse peritoneal inflammation (peritonitis), or formation of an abscess (collection of pus). • Usually manifests with worsening abdominal pain over time, high fever, absence of bowel movements, nausea or vomiting, and general intoxication. • Symptom development is more rapid and the course is more severe. |
Acute diverticulitis is a clinically urgent condition, and in this case medical advice or care at a healthcare facility providing emergency care must be sought immediately. By performing an objective assessment and the additionally required investigations, it is possible to evaluate the severity of diverticulitis and decide on the necessary treatment.
Diverticulosis is most often identified as an incidental finding during colonoscopy or during computed tomography (CT) examination of the abdominal cavity for another reason. If acute diverticulitis is suspected, colonoscopy must not be performed due to the risk of intestinal perforation (rupture). In this case, the diagnosis is confirmed based on the characteristic clinical signs and radiological findings (usually by performing CT).
Surgical treatment is indicated in cases of acute complicated diverticulitis when the existing clinical situation cannot be resolved conservatively. In this case, an open-type operation (laparotomy) with removal of the inflamed intestinal segment (colon resection) is most often performed. Because of the acute process, the operation is often completed by bringing the intestine out onto the anterior abdominal wall, i.e., creation of a stoma.
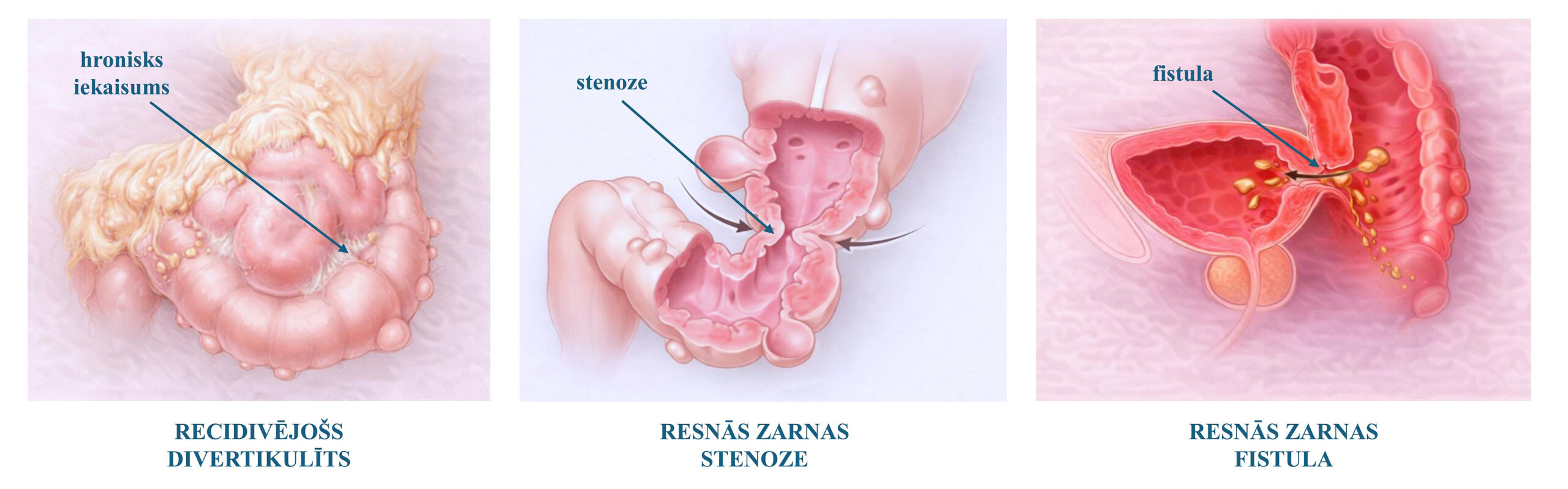
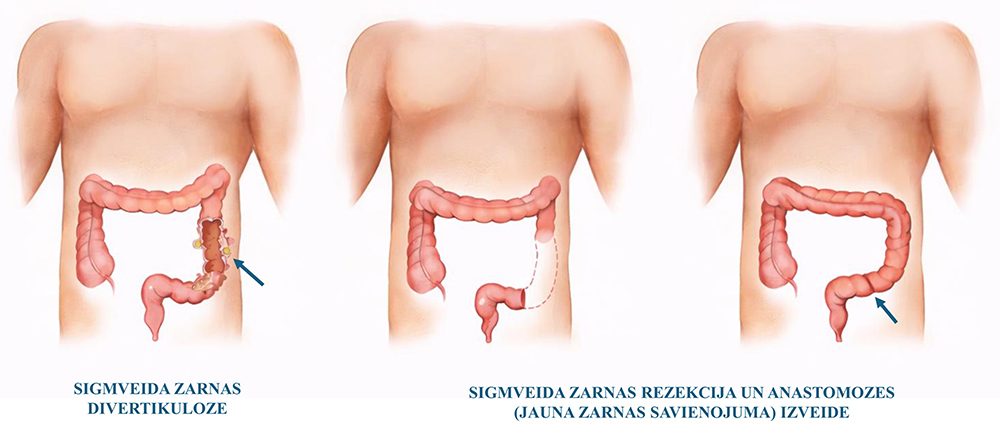
In cases where recurrent diverticulitis is observed, surgical treatment in an elective setting should be considered. Indications are determined by the patient's current quality of life, intensity of complaints, as well as investigation findings. The aim of elective surgery is to eliminate the chronic inflammatory process and protect against the possible future development of complicated diverticulitis. The operation is most often performed laparoscopically (in a minimally invasive manner), and during it the entire anatomically altered part of the colon (where diverticula are found) is removed. A new colon connection is created, which allows bowel movements to be maintained via the natural route (Figure 3).
If chronic complications associated with previous diverticulitis (stenosis, fistula) have developed, surgical treatment is recommended in all cases, considering that they cannot be resolved with conservative treatment methods.









CALL US:
+371 26 412 412WHATSAPP:
+371 26 412 412
If you need an appointment before surgery, please let us know when calling —
we will offer you the earliest available appointment.
SEND US A MESSAGE

