
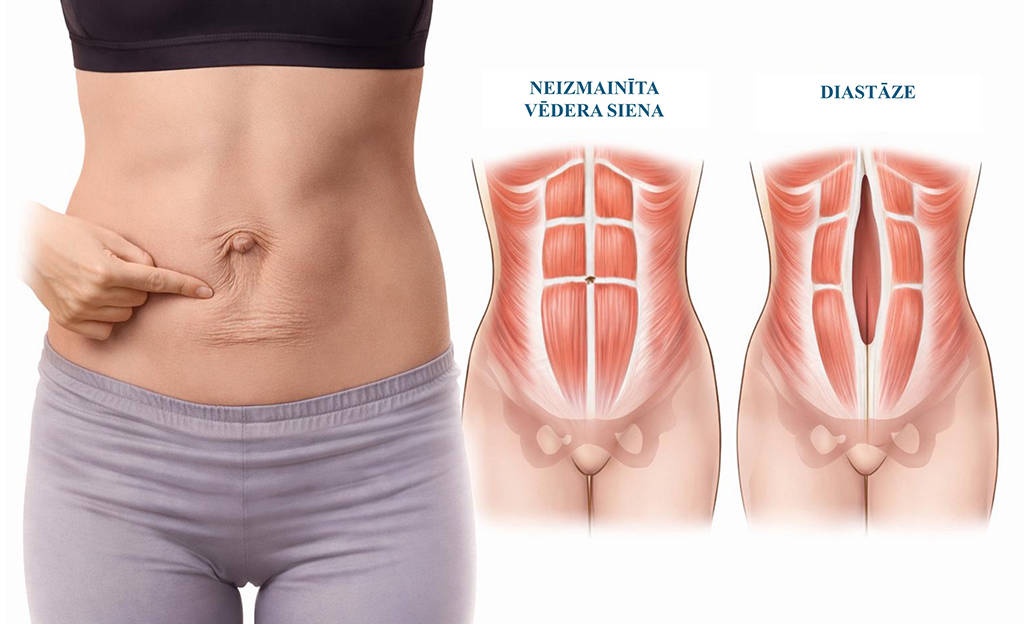
Diastasis is a condition in which a gap forms along the abdominal midline between the rectus muscles of the anterior abdominal wall, causing abdominal wall weakness (Figure 1). Diastasis is not a hernia, because there is no fascial defect (in the connective tissue layer of the abdominal wall), although both conditions may coexist.
Diastasis is promoted by several factors: pregnancy, obesity, heavy physical exertion (incorrect technique) and ageing (weakening of connective tissue).
For more precise assessment and measurement of diastasis, ultrasonography (US) is used, usually ordered by a specialist.
Complaints are most often cosmetic and functional. A dome-shaped protrusion appears in the abdominal midline during exertion or changes in body position, and persistent body-contour changes may develop. Because abdominal wall weakness affects core stability, more pronounced diastasis may be accompanied by postural disorders, low back pain, pelvic floor muscle dysfunction (pelvic heaviness, urinary incontinence), increased bloating after meals and difficulty with daily physical activities. Diastasis also increases the risk of an abdominal wall hernia.
Treatment of diastasis is gradual and depends on symptoms, diastasis width and the patient's goals. The two main approaches are conservative therapy (physiotherapy) and surgical treatment.
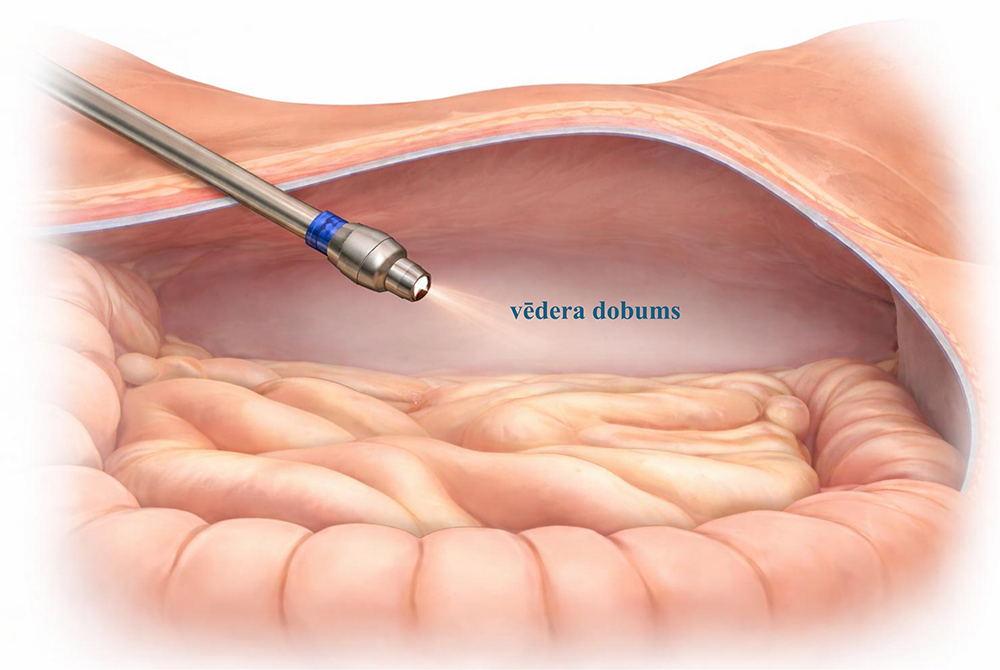
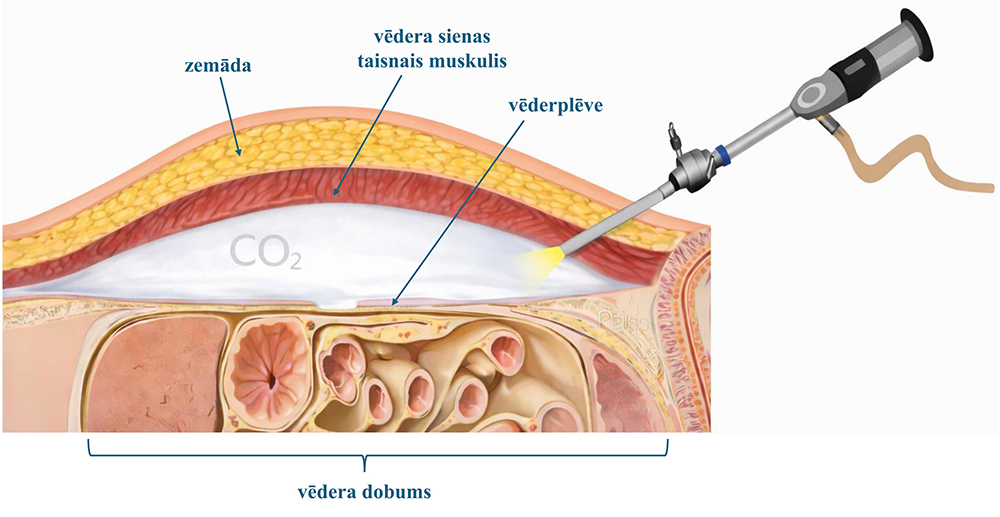
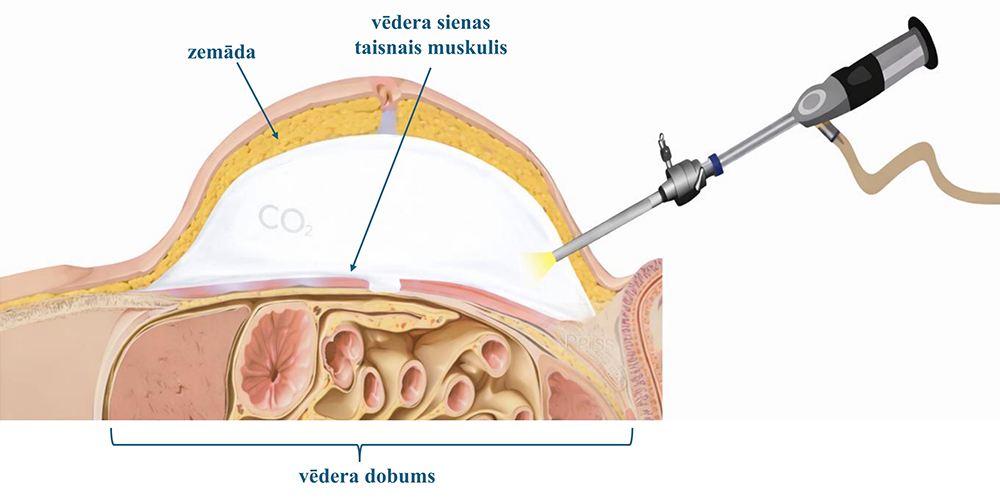
The main surgical methods for diastasis correction are laparoscopic and conventional (open) approaches. The aim is to suture the edges of the rectus muscles of the anterior abdominal wall together while correcting an abdominal wall hernia if present. Technique choice depends on abdominal wall tissue quality, diastasis width and coexisting hernias. Usually, a synthetic mesh is inserted to strengthen the abdominal wall and reduce the risk of diastasis recurrence (reformation) (Figure 2).

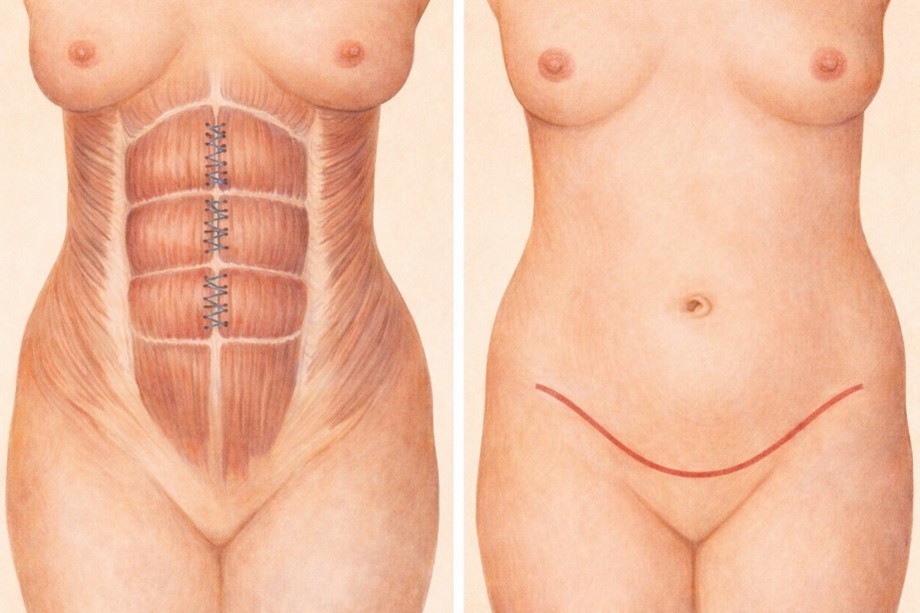
Conventional or open surgery for correction of diastasis (if the only aim is to eliminate the abdominal wall defect) is performed much less often, because minimally invasive approaches are the current standard of care for diastasis. If excess abdominal skin must also be removed (abdominoplasty), correction of diastasis and hernias can be performed at the same time (Figure 6).









CALL US:
+371 26 412 412WHATSAPP:
+371 26 412 412
If you need an appointment before surgery, please let us know when calling —
we will offer you the earliest available appointment.
SEND US A MESSAGE

